Systematic reviews and meta-analyses are pivotal for evidence-based decision-making but depend on the availability of precise statistical data. Researchers often encounter studies where essential statistics are missing or presented only in graphs, leading to potential data exclusion and selection bias. This study aims to provide specific methodologies for extracting or reconstructing the statistical parameters required for meta-analysis—specifically effect sizes (MD, OR, RR, HR) and their corresponding variance measures (SD, SE, variance)—from incomplete or graphically reported data. We describe calculation and extraction protocols for five specific scenarios encountered in medical literature: (1) continuous data missing standard deviations; (2) categorical data missing standard errors; (3) calculating risk estimates from frequency tables; (4) extracting continuous data presented solely in graphs; and (5) reconstructing hazard ratios from Kaplan-Meier survival curves. Valid meta-analysis requires both an effect size and a measure of variance. When these are not explicitly reported, they can often be derived from other available statistics or digital extraction from figures. While heterogeneity is inherent in meta-analysis, the methodology allows for error adjustment and robust synthesis. Therefore, preventing data loss via these extraction methods is preferable to excluding studies. Maximizing data inclusion enhances the comprehensive value and statistical power of the final analysis.
Clinical practice guidelines (CPGs) are critical for translating research into clinical practice; however, high-quality evidence alone does not ensure optimal care. The integration of patient values and preferences is essential for developing recommendations that are both relevant and applicable, yet many guidelines continue to underrepresent patient perspectives and lack transparent incorporation of preference research. This review delineates the distinction between values and preferences, examines their influence on preference-sensitive decisions, and evaluates methods for eliciting patient input, such as utility-based measurements, discrete-choice experiments, and qualitative studies. Systematic integration of this evidence through guideline development enhances both credibility and patient-centeredness. Persistent challenges include issues of representativeness, methodological uncertainty, and cultural barriers. Implementing practical strategies to address these challenges will improve transparency, relevance, and acceptance of clinical practice guidelines.
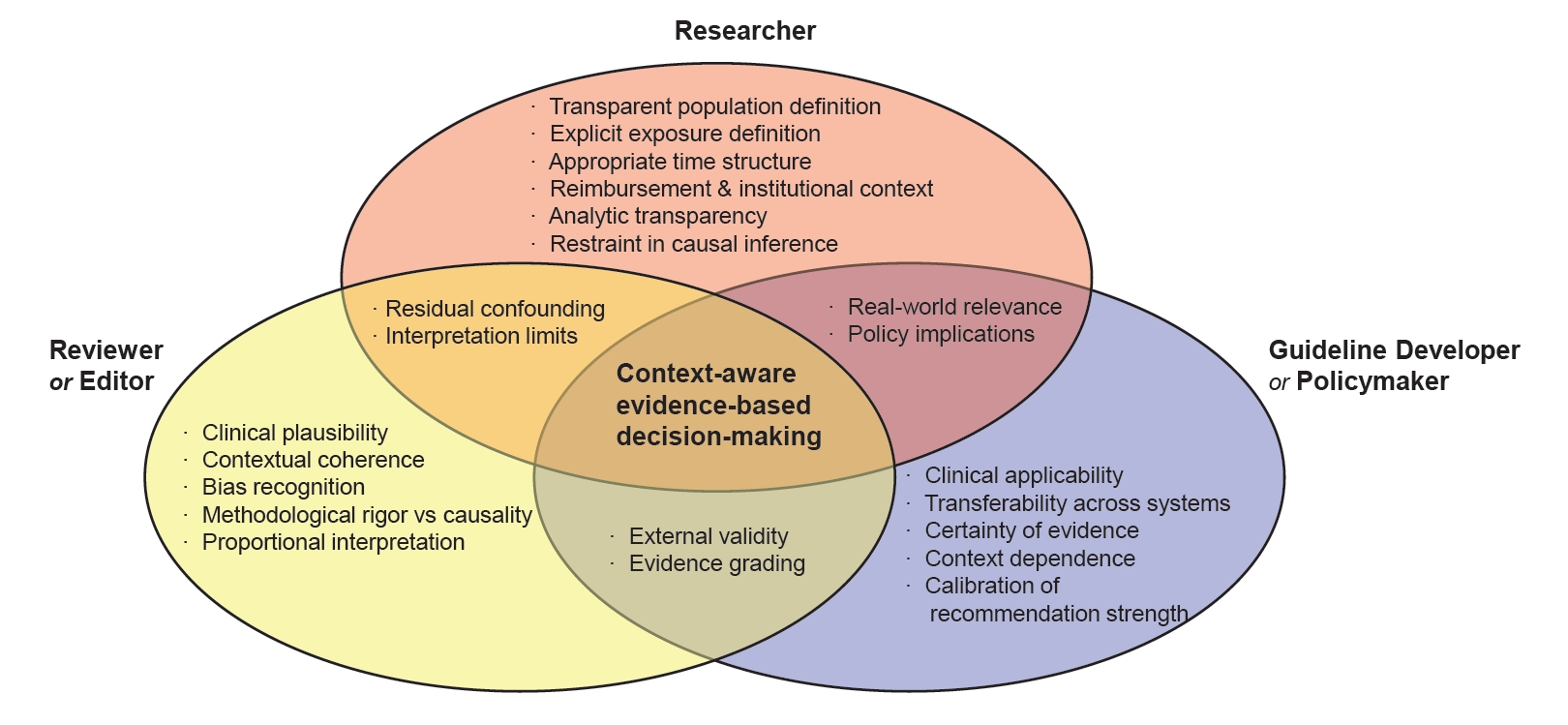
Big data–driven non-randomized studies (NRS) are an increasingly important source of observational evidence in evidence-based medicine, particularly when randomized controlled trials are limited, infeasible, or insufficiently generalizable to routine clinical practice. In Korea, this shift is especially pronounced because a single-payer national health insurance system enables near-complete population coverage, longitudinal follow-up, and linkage of healthcare utilization, prescriptions, and mortality data. These structural advantages, however, also create distinctive interpretative challenges. In big data–based NRS, flexible choices in population definition, exposure classification, index dates, follow-up windows, and outcome specification—together with reimbursement-driven healthcare utilization, frequent policy changes, rapid demographic aging, and evolving standards of care—can render observed associations vulnerable to residual confounding and overinterpretation. Advanced analytic approaches may improve internal validity, but they cannot fully resolve ambiguities related to population specification, temporal structure, or unmeasured contextual factors. This review discusses how to interpret big data–driven NRS using the Korean healthcare system as a representative example. We summarize the strengths that make large-scale observational research indispensable, delineate structural, institutional, and temporal factors that complicate causal inference, and propose practical principles for responsible interpretation. We emphasize the complementary responsibilities of researchers, reviewers and editors, and guideline developers in supporting transparent design, clinically plausible interpretation, and calibrated use of observational evidence in recommendations. A context-aware and proportionate approach is essential to ensure that expanding observational evidence strengthens—rather than distorts—evidence-based clinical and policy decision-making in rapidly evolving healthcare systems with complex institutional incentives.
Background Post-thyroidectomy hypocalcemia is the most frequent complication after total thyroidectomy. Preoperative vitamin D deficiency has been suggested as a potential risk factor, but inconsistencies exist in the literature, possibly related to methodological differences. To evaluate whether study design and risk of bias influence the association between preoperative vitamin D deficiency and postoperative hypocalcemia in patients undergoing total thyroidectomy.
Methods This is a secondary analysis of a previously conducted systematic review. We included observational studies evaluating the association between preoperative vitamin D levels and postoperative hypocalcemia. Methodological quality was assessed using the QUIPS tool. Subgroup analyses were performed based on study design (prospective vs. retrospective) and overall risk of bias (high vs. low/moderate).
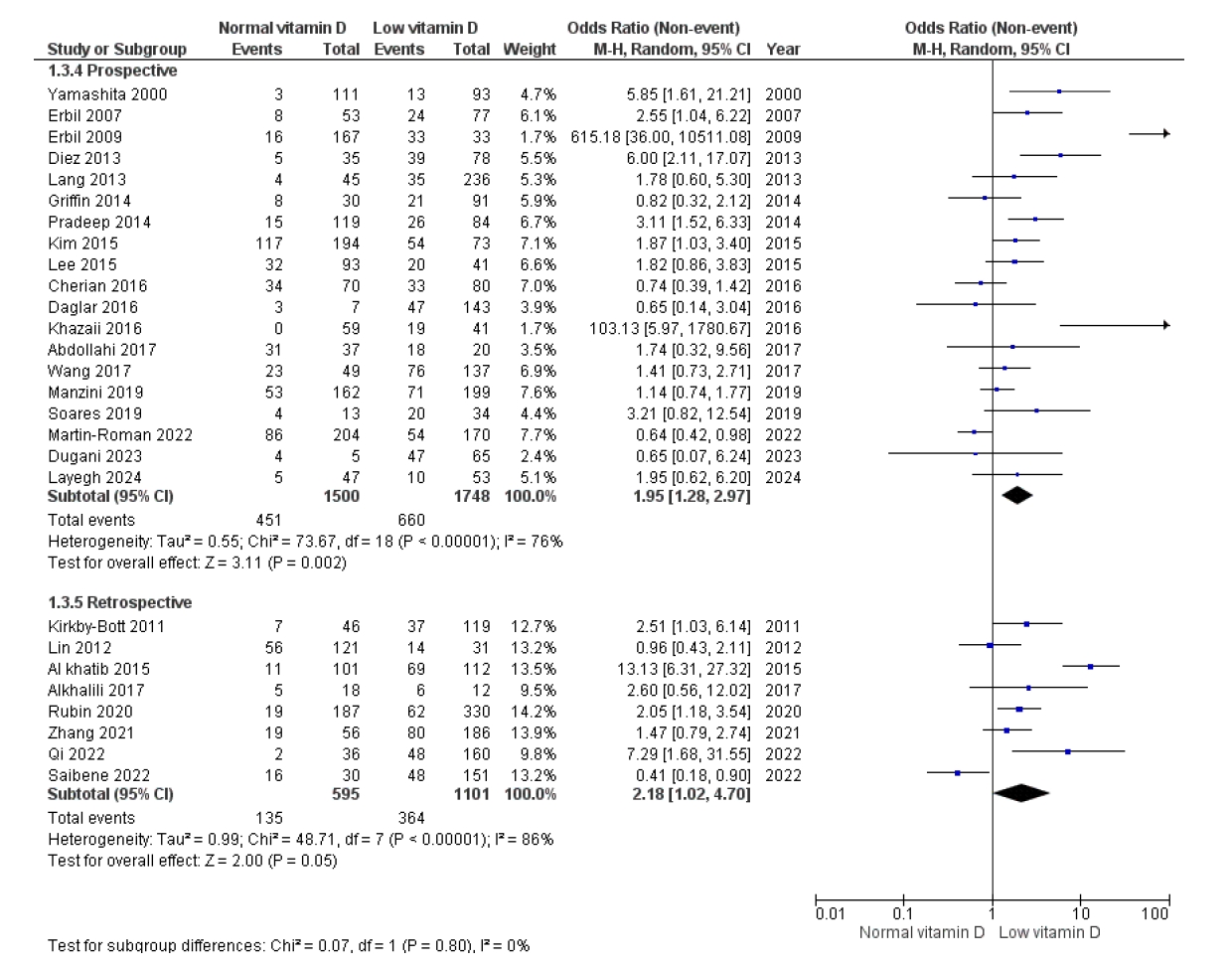
Results Twenty-eight studies comprising 4994 patients were included. Nineteen studies had a prospective design. Both prospective and retrospective studies showed an association between vitamin D deficiency and hypocalcemia; however, the effect size was lower in prospective studies (OR 1.95; 95% CI 1.28-2.97) compared to retrospective ones (OR 2.18; 95% CI 1.02-4.7). Studies with high risk of bias showed a significant association (OR 2.55; 95% CI 1.4-3.6), while those with low/moderate risk did not (OR 1.71; 95% CI 0.96-3.06).
Conclusion Study design and methodological quality influence the reported association between vitamin D deficiency and postoperative hypocalcemia. These findings suggest caution when recommending preoperative vitamin D supplementation based solely on observational data.




 First
First Prev
Prev

