This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clinical practice guidelines (CPGs) are critical for translating research into clinical practice; however, high-quality evidence alone does not ensure optimal care. The integration of patient values and preferences is essential for developing recommendations that are both relevant and applicable, yet many guidelines continue to underrepresent patient perspectives and lack transparent incorporation of preference research. This review delineates the distinction between values and preferences, examines their influence on preference-sensitive decisions, and evaluates methods for eliciting patient input, such as utility-based measurements, discrete-choice experiments, and qualitative studies. Systematic integration of this evidence through guideline development enhances both credibility and patient-centeredness. Persistent challenges include issues of representativeness, methodological uncertainty, and cultural barriers. Implementing practical strategies to address these challenges will improve transparency, relevance, and acceptance of clinical practice guidelines.
Clinical practice guidelines (CPGs) are systematically developed statements intended to support optimal clinical decision-making by translating appraised and synthesized evidence into actionable recommendations. With the growing emphasis on patient-centered care within health systems, guideline developers are increasingly expected to involve patients in priority setting and to ensure that recommendations reflect patient priorities in both everyday life and clinical practice.
Incorporating patient values and preferences into guidelines can enhance their feasibility and acceptability in clinical practice [1,2]. Excluding patient perspectives may result in recommendations that overlook individual circumstances and trade-offs, potentially leading to reduced adherence [3]. Mirza et al. emphasized that involving patient panels through structured approaches can help guideline developers prioritize outcomes that matter to patients, extending beyond traditional clinical endpoints [4].
Contemporary guideline development standards increasingly recognize patient values and preferences as a core component of trustworthy recommendations [5]. However, empirical evaluations indicate that patient involvement and the systematic use of preference research remain inconsistent and are frequently inadequately documented in final guideline products [6]. This inconsistency is partly due to the tendency to treat preferences as subjective inputs rather than as an evidence domain that can be systematically identified, appraised, and synthesized, as well as the lack of practical guidance on integrating preference evidence. To provide a clear framework for readers, this review will first clarify the conceptual distinction between values and preferences, then explain the pivotal role of preference evidence in preference-sensitive decisions and finally summarize feasible methods and stage-specific strategies for integrating patient perspectives into guideline development.
Conceptual Definitions of Patient Values and Preferences
The term ‘patient preferences’ is applied heterogeneously, encompassing at least two levels: (1) individual choices made during clinical encounters and (2) aggregate evidence about preferences derived from population-based studies. Failure to distinguish between these levels can lead to confusion when searching for, synthesizing, and reporting preference-related evidence.
Patient values are defined as the relative importance patients assign to outcomes, health states, and treatment attributes, such as symptom relief, survival, adverse effects, cost, and burden. Patient preferences are defined as expressed choices or rankings among reasonable alternatives, reflecting how patients weigh these valued outcomes and attributes in specific contexts. Preferences thus operationalize values into concrete decisions.
Although values and preferences are conceptually distinct—with values describing the importance of outcomes and preferences describing choices among alternatives—the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach often integrates these constructs. Within GRADE, 'patient values and preferences' are typically operationalized as the relative importance assigned to outcomes or health states of interest [7]. Whether an intervention is preferred depends on how patients weigh benefits, harms, costs, and treatment burden [8]. Even when population-level evidence indicates general trends, individual contexts and goals may differ. Therefore, guidelines should clearly distinguish between typical patterns in the target population and the necessity for individualized application in clinical practice [9].
Importance of Incorporating Patient Values in Guideline Development
Incorporating patient values and preferences into CPGs is fundamental to patient-centered care and enhances the reception and implementation of recommendations. In individual clinical encounters, explicit consideration of patient priorities supports more tailored and higher-quality decisions [10]. Even when clinical effectiveness evidence is equivalent, the preferred option may differ based on a patient’s priorities and tolerance for risk or burden.
Clinicians' preferred treatments, chosen for their effectiveness, may not always align with patients' priorities. Owens et al. demonstrated that patient preferences could alter recommendations for spinal disease treatment, as patients and clinicians may assess risks and benefits differently [3]. Uniform recommendations that disregard preference heterogeneity may therefore result in suboptimal outcomes. When a recommendation conflicts with a patient’s values, intentional non-adherence may occur; such decisions should not be automatically interpreted as poor-quality care, as they may represent value-concordant choices [11].
Guidelines that transparently articulate value judgments can reduce expectation gaps between patients and clinicians, thereby facilitating more effective shared decision-making (SDM) by clarifying which outcomes and trade-offs should be discussed during consultations [12]. When appropriate, supplementing recommendations with plain-language summaries and decision aids can further enhance understanding and support implementation.
Preference-sensitive Decisions
As used here, values refer to the relative importance patients assign to outcomes and attributes, whereas preferences refer to expressed choices or rankings among reasonable alternatives that follow from those values.
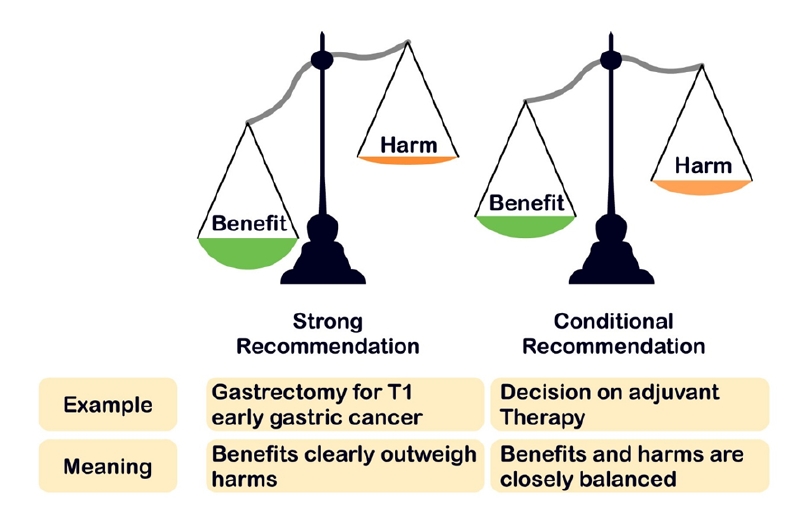
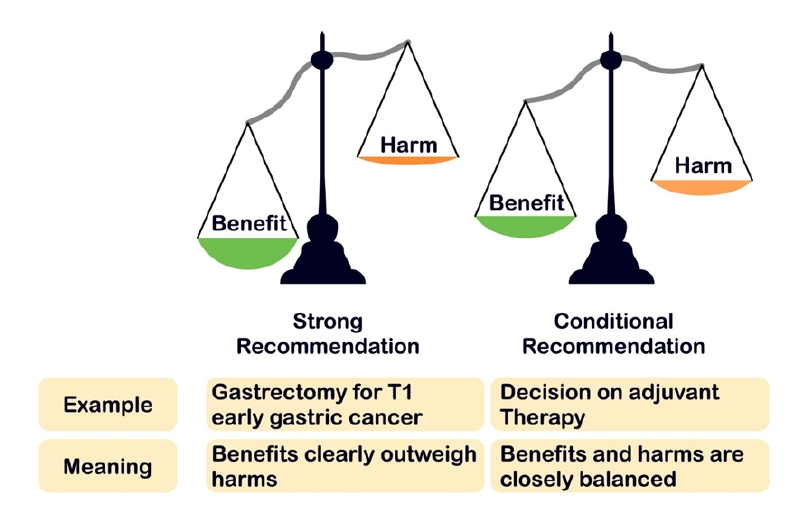
Within the GRADE methodology, the strength of a recommendation is determined not only by the certainty of evidence but also by the balance between benefits and harms and the degree of variability in patient values and preferences (Fig. 1). When patient values are broadly consistent and the benefit–harm balance is clear, strong recommendations are justified. Conversely, when the balance is closely matched or values vary substantially, conditional recommendations are more appropriate. In these cases, guidelines should explicitly indicate the need to elicit individual preferences through SDM in clinical practice.
Many clinical choices are preference-sensitive decisions, characterized by the existence of multiple reasonable alternatives and meaningful trade-offs in burden, risks, or quality of life, such that the optimal option depends on patient value judgments [13]. In these contexts, even with sufficient effectiveness evidence, different conclusions may be reasonable depending on which outcomes are prioritized [14]. Guideline developers should therefore actively seek and incorporate preference evidence during development and reflect anticipated variability in the rationale and wording of recommendations.
Evidence suggests that clinicians frequently have difficulty accurately predicting which outcomes patients prioritize, such as quality of life versus survival duration or tolerance of specific risks [15,16]. Therefore, guidelines should move beyond reporting general trends and provide concrete prompts to facilitate preference elicitation at key decision points, such as suggested questions to explore patient goals, concerns, and acceptable trade-offs.
Gartner et al. analyzed oncology CPGs modules in the Netherlands and found that 18 of 32 recommendations were preference-sensitive; notably, 3 of 14 recommendations presented as strong would have been more appropriately classified as conditional based on the underlying text [17]. They argued that standard guideline phrasing may be insufficient to foster choice awareness or to encourage neutral presentation of options in clinical discussions [17]. These findings support the recommendation that guideline wording should explicitly acknowledge legitimate alternatives where preference sensitivity is anticipated and direct clinicians to verify patient values, even when recommendations are strongly framed.
The presence of a strong recommendation does not eliminate the need for SDM. Even when a strong recommendation is issued, an alternative option may be rational if the patient’s context and goals differ. The perspective that patient participation is only necessary for conditional recommendations has been criticized as inconsistent with patient-centered care [9].
Current Status of Patient Involvement in Guidelines and Gaps
Despite broad consensus on the importance of patient values and preferences, evaluations repeatedly show that patient/public involvement and the systematic use of preference evidence remain limited and inconsistently applied in guideline development. International reviews suggest that approximately half of major guideline organizations report routine patient involvement, indicating substantial variability in practice.
Armstrong et al. reviewed 101 independent recommendation-developing organizations in the United States (2011–2015) using websites, methodology manuals, and guideline documents and found that only 8% required patient/public participation in guideline development groups, while 15% described it as optional or occasional [18].
Evidence also suggests that patient participation can materially change the scope and content of guidelines. For example, parallel guideline development groups, with and without patient representatives, identified additional outcomes important to patients (e.g., trajectories of cognitive decline and the speed of disease progression) and shifted discussion toward a patient-centered framing [19]. Such involvement may influence outcome selection, the direction and strength of recommendations, and dissemination strategies, ultimately strengthening acceptability and implementability [19].
In an earlier survey of 31 international guideline developers, 58% reported including patients on panels and 45% reported using surveys to assess patient preferences [20]. Even after influential recommendations by the Institute of Medicine (now the National Academy of Medicine), subsequent analyses indicate that meaningful patient participation remains suboptimal in many guideline programmes [18,21].
Beyond direct participation, available analyses reveal persistent gaps in the use and reporting of preference research evidence in both pharmaceutical coverage decisions and CPGs development [22]. Content analyses underscore this issue, showing that guideline documents allocate substantially less attention to patient preferences than to clinical effectiveness evidence. For instance, Chong et al. observed that effectiveness evidence comprised 24.2% of guideline text, whereas patient preference content comprised only 4.6%, with preference studies rarely cited [23]. Similarly, Sale et al. reported that among 70 international osteoporosis guidelines, only 39% explicitly mentioned patient beliefs, values, or preferences, and most of these did not support their recommendations with evidence from primary studies or systematic reviews [24]. Taken together, these studies highlight a consistent gap: guidelines often acknowledge the relevance of patient preferences yet fall short of systematically incorporating and reporting empirical preference evidence in decision-making.
Finally, guideline documents often fail to report concretely how panels weighed patient values and preferences when judging benefit–harm trade-offs [25]. Armstrong et al. noted that many studies focus on exploratory descriptions of methods; few empirically evaluate how patient participation affects question formulation and recommendation development [19].
Barriers to Patient Involvement in Guideline Development
Commonly reported barriers to meaningful patient participation include resource constraints (time, budget, personnel), recruitment challenges, concerns about representativeness, limited health literacy and difficulties understanding technical evidence, resistance from developers or panel members, and inadequate facilitation and communication capacity [14,18].
Additional barriers arise from conceptual ambiguity. Terminology around “patient preference” is used inconsistently across stakeholders, complicating evidence searching and synthesis. Moreover, panels often lack explicit guidance on how much weight preference evidence should receive relative to other decision criteria such as effectiveness, cost, feasibility, and equity [26]. Methodology manuals frequently do not provide sufficient operational procedures or reporting templates for integrating preference evidence into deliberations and documenting its influence on recommendations [6,27].
Structural inequities and culture can further limit participation. Socioeconomic constraints, educational disparities, and persistent expert-centric norms may exclude underrepresented groups and marginalized patient input even when involvement is formally encouraged [5]. Addressing these barriers requires both procedural improvements (e.g., recruitment strategies, support and training, compensation) and cultural change that treats patient perspectives as essential evidence for trustworthy guidance.
Types of Patient Preference Evidence and Measurement Methodologies
Approaches for incorporating patient perspectives in guidelines can be grouped into (1) direct patient and public involvement (e.g., Guideline Development Group (GDG) membership, focus groups, public comment, patient panels) and (2) the use of preference evidence derived from research on patient values and preferences (Table 1), which can be used as a quick reference to match research methods with specific guideline development needs.
Regarding the latter, research methodologies are commonly distinguished into four categories. Qualitative methods (e.g., in-depth interviews) are valuable for identifying outcomes and explaining the decision factors important to patients [28]. Quantitative surveys (e.g., Likert scales, visual analogue scales (VAS)) help quantify relative importance but may limit the assessment of complex trade-offs. To explicitly model these trade-offs, preference elicitation techniques such as Discrete Choice Experiments (DCE) are essential; for instance, Mühlbacher et al. (2021) used a DCE to identify avoidance of severe hypoglycemia as a dominant preference relative to other attributes [29]. Finally, utility measurements (e.g., Standard Gamble) derive values required for economic evaluations.
Since preferences may concern care processes as well as outcomes [26], mixed-methods designs are often recommended. These approaches allow researchers to generate candidate attributes through qualitative work and then estimate weights and explore heterogeneity through quantitative studies [28,30].
Incorporating Patient Values and Preferences at Each Guideline Development Stage
Integrating patient values and preferences at each stage of the CPGs development process involves a sequence of coordinated steps. Begin by identifying "questions/outcomes important to patients" during the scoping phase. Then, conduct a targeted search for preference evidence to connect with Evidence-to-Decision (EtD) discussions. Structurally reflect patient perspectives during the consensus process and explicitly state preference sensitivity, with supporting materials, in the final product. This systematic approach embeds patient perspectives at every key stage.
Scoping and question formulation
Early incorporation of patient input is critical to prevent guideline priorities from diverging from lived experiences. Needs assessments, public surveys, and focus group interviews can identify outcomes and decision factors that patients consider most important [31]. Using this information to refine Population–Intervention–Comparator–Outcome (PICO) questions and to prioritize key outcomes reduces the risk of overlooking quality-of-life outcomes or longer-term concerns. Including patients or patient representatives in the GDG further increases the likelihood that outcomes clinicians may underweight are incorporated into the scope [19].
Evidence review stage – collection of preference-related evidence
In the evidence review stage, panels should use explicit procedures to identify and appraise preference-related evidence separately from clinical effectiveness evidence [10]. The GRADE EtD framework includes a values and preferences domain, encompassing outcome importance, risk acceptance, and perspectives on treatment burden [32]. Zhang et al. described guideline development processes in which additional searches were performed for preference literature (e.g., utility values, quality of life data, treatment preference surveys, qualitative research) for each PICO question and were then incorporated into EtD discussions with input from clinicians and patient representatives [10]. Because preference evidence may be sparse for specific subpopulations or regions, developers may need to prioritize local evidence and, where feasible, complement gaps with targeted qualitative studies or surveys.
Recommendation formulation stage – patient panel involvement and panel surveys
During recommendation formulation and consensus, governance structures should enable patient perspectives to influence deliberations substantively. Direct patient or patient-representative membership on GDGs is the most transparent approach, while a separate patient panel can provide structured input at critical decision points [27,31]. Meaningful participation requires clear recruitment criteria, attention to representativeness, preparatory education and support, appropriate compensation, and skilled facilitation. Providing plain-language materials and flexible participation modalities (e.g., online or asynchronous formats) can help mitigate barriers associated with educational and socioeconomic disparities [5].
Goodman et al. illustrated that a rheumatoid arthritis patient panel’s prioritization of trade-offs between infection risk and relapse risk could shift the direction and strength of recommendations toward conditional recommendations [14]. When direct participation is infeasible, structured procedures such as panel surveys can supplement deliberations. Zeng et al. proposed a survey framework to elicit and share patient perspectives (e.g., minimum acceptable benefit, risk tolerance) before meetings [30]. Because expert estimation may not fully reflect patient experience, such approaches should be triangulated with empirical patient data whenever possible.
Recommendation wording & supplementary materials – explicit statement of preference information
In drafting recommendations and accompanying materials, panels should: (1) explicitly indicate when decisions are preference-sensitive and specify reasonable exceptions; (2) summarize the key preference evidence and its variability; and (3) provide tools that support SDM (e.g., plain-language summaries, decision aids). Brief summaries of what patients value most (and the extent of variability) can facilitate evidence-based dialogue during consultations. Citing preference instruments or primary preference studies in recommendation rationales can also make transparent how patient perspectives were considered [33]. As Gartner et al. argued, recommendation phrasing should promote choice awareness when multiple reasonable options exist [17].
Remaining Challenges and Potential Solutions
Despite the emerging methodologies for integrating patient values and preferences into CPGs, several impediments remain. Implementing these concepts requires overcoming concerns regarding representativeness, resource constraints, methodological uncertainties, cultural resistance, and the need for patient empowerment.
A primary concern is the representativeness of patient opinions. Since individual preferences vary significantly by disease stage, age, socioeconomic background, and culture, a limited number of patient panelists may not adequately reflect the universal values of the target population. To mitigate this limitation, guideline developers should strive to include patients from diverse backgrounds and utilize multiple channels, such as surveys and focus groups, to gather a broader range of perspectives. Furthermore, integrating large-scale survey data and systematic literature reviews can supplement direct participation. As demonstrated by Goodman et al., while acknowledging the constraints of small panels, triangulating panel discussions with existing literature evidence can lead to more persuasive and representative value judgments [14].
Practical constraints—including time, budget, and personnel—can hinder implementation. Overcoming these barriers requires early planning and resource allocation. Securing funds for recruitment, travel, and honoraria, as well as providing facilitators, patient coordinators, and educational resources, supports meaningful participation [5]. While these steps require investment, they increase the long-term acceptability and usefulness of guidelines. Institutional support, such as dedicated budget items for patient involvement, is also essential.
Methodological uncertainty further complicates the integration process [26]. As noted by Kim et al., there is a lack of consensus on the optimal methods for integrating and reporting preference evidence, and relevant studies remain scarce [27]. To bridge this gap, it is essential to systematically document and evaluate the success and failure factors of various engagement strategies in guideline development. Sharing these experiences through international platforms such as the Guidelines International Network (GIN) and conducting local primary research—both quantitative and qualitative—will strengthen the evidence base. For instance, discrepancies in attitudes toward end-of-life care planning among patients, families, and physicians highlight the need for region-specific data to inform policy and guideline development.
Cultural barriers and the need for a paradigm shift present another formidable challenge. In medical cultures where expert opinion is traditionally prioritized, patient preferences may be marginalized even if their consideration is mandated by guidelines. Overcoming this requires continuous education for healthcare professionals to reinforce that respecting patient values is central to high-quality care. Armstrong et al. argue that patient participation should be regarded as a prerequisite for the trustworthiness of guidelines [19].
Finally, effective integration depends on patient empowerment. Patients must be able to voice their opinions and participate meaningfully in the decision-making process. This can be achieved by improving health literacy and access to information. Furthermore, structured training programs for patient representatives, like those operated by the National Institute for Health and Care Excellence (NICE), can significantly enhance the quality of patient contributions. Ultimately, establishing a "co-production" model where patients and clinicians act as partners will be instrumental in fostering a truly patient-centered medical culture.
Conclusion
Systematically integrating patient values and preferences into CPGs development can strengthen the relevance, acceptance, and practical implementation of recommendations. To achieve this, guideline developers should: (1) distinguish values (outcome and attribute importance) from preferences (choices and trade-offs); (2) identify, appraise, and synthesize preference evidence alongside effectiveness evidence; and (3) transparently document how preference evidence informed EtD deliberations, recommendation wording, and the need for SDM at preference-sensitive decision points. In practical terms, developers can apply a stepwise approach by beginning with patient inclusion on guideline panels and progressively incorporating broader surveys, focus groups, or mixed-methods preference studies as resources permit. By tailoring the level of patient involvement to the specific context and available resources, guideline developers can more effectively ensure that recommendations are both feasible to implement and closely aligned with the lived experiences and priorities of the patient population.
Interpretation of recommendation strength within the GRADE framework.
Strong recommendations are appropriate when expected benefits clearly outweigh harms and patient values and preferences are relatively consistent. Conditional recommendations are appropriate when benefits and harms are closely balanced and/or when values and preferences are expected to vary, signaling the need for shared decision-making. Examples shown are illustrative and not intended to be prescriptive: gastrectomy for T1 early gastric cancer (strong) and decision on adjuvant therapy (conditional).
Table 1.
Types and Characteristics of Patient Values and Preferences Research Methods
Category
Method
Characteristics & Description
Key Outcome / Measure
Qualitative Methods
In-depth Interview
Explores individual experiences, values, and contextual backgrounds in detail. Useful for discovering novel value drivers.
Key concepts and value categories (Thematic analysis)
Focus Group Discussion (FGD)
Identifies shared opinions or conflicting views through group interaction. Often used for instrument development.
Group dynamics, consensus, and spectrum of perspectives
Quantitative Survey
Likert Scale
Measures level of agreement or importance using an ordinal ranking scale. Low cognitive burden and intuitive.
Mean scores, frequency distribution, response rates
Visual Analogue Scale (VAS)
Quantifies subjective value by asking respondents to mark their preference state on a continuous line (e.g., 0–100).
Mean score (0–100 scale), median values
Preference Elicitation
Discrete Choice Experiment (DCE)
Analyzes trade-offs by requiring respondents to choose between hypothetical scenarios defined by varying attributes and levels.
Part-worth utility, relative importance, marginal rates of substitution
Best-Worst Scaling (BWS)
Measures preference intensity by asking respondents to select the "best" (most important) and "worst" (least important) items.
Preference scores, relative importance rankings
Utility Measurement
Standard Gamble (SG)
Measures health state utility based on decision-making under uncertainty (risk).
Utility values (0–1), basis for quality-adjusted life year (QALY) calculation
Time Trade-Off (TTO)
Measures utility by determining the indifference point between a duration in a specific health state and a shorter duration in perfect health.
Utility values, weights for quality-adjusted life year (QALY) calculation
References
1. Sleath B, Carpenter DM, Slota C, Williams D, Tudor G, Yeatts K, et al. Communication during pediatric asthma visits and self-reported asthma medication adherence. Pediatrics 2012; 130: 627-33.
2. Cronin RM, Mayo-Gamble TL, Stimpson SJ, Badawy SM, Crosby LE, Byrd J, et al. Adapting medical guidelines to be patient-centered using a patient-driven process for individuals with sickle cell disease and their caregivers. BMC Hematol 2018; 18: 12.
4. Mirza RD, Bolster MB, Johnson SR, Allen A Jr, Bernstein EJ, Chung JH, et al. Assessing patient values and preferences to inform the 2023 American College of Rheumatology/American College of Chest Physicians interstitial lung disease guidelines. Arthritis Care Res (Hoboken) 2024; 76: 1083-9.
5. Loyola G, Morales D, Leyton F, Alonso-Coello P, Bracchiglione J. Incorporating patients in the development of clinical practice guidelines. Medwave 2025; 25: e3063.
6. Selva A, Sanabria AJ, Pequeno S, Zhang Y, Sola I, Pardo-Hernandez H, et al. Incorporating patients' views in guideline development: a systematic review of guidance documents. J Clin Epidemiol 2017; 88: 102-12.
7. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008; 336: 924-6.
8. Schunemann HJ, Wiercioch W, Etxeandia I, Falavigna M, Santesso N, Mustafa R, et al. Guidelines 2. 0: systematic development of a comprehensive checklist for a successful guideline enterprise. CMAJ 2014; 186: E123-42.
9. Mercuri M, Baigrie BS, Gafni A. Patient participation in the clinical encounter and clinical practice guidelines: the case of patients' participation in a GRADEd world. Stud Hist Philos Sci 2021; 85: 192-9.
10. Zhang Y, Coello PA, Brozek J, Wiercioch W, Etxeandia-Ikobaltzeta I, Akl EA, et al. Using patient values and preferences to inform the importance of health outcomes in practice guideline development following the GRADE approach. Health Qual Life Outcomes 2017; 15: 52.
11. Arts DL, Voncken AG, Medlock S, Abu-Hanna A, van Weert HC. Reasons for intentional guideline non-adherence: a systematic review. Int J Med Inform 2016; 89: 55-62.
14. Goodman SM, Miller AS, Turgunbaev M, Guyatt G, Yates A, Springer B, et al. Clinical practice guidelines: incorporating input from a patient panel. Arthritis Care Res (Hoboken) 2017; 69: 1125-30.
15. Pieterse AH, Baas-Thijssen MC, Marijnen CA, Stiggelbout AM. Clinician and cancer patient views on patient participation in treatment decision-making: a quantitative and qualitative exploration. Br J Cancer 2008; 99: 875-82.
16. Hamelinck VC, Bastiaannet E, Pieterse AH, Jannink I, van de Velde CJ, Liefers GJ, et al. Patients' preferences for surgical and adjuvant systemic treatment in early breast cancer: a systematic review. Cancer Treat Rev 2014; 40: 1005-18.
17. Gartner FR, Portielje JE, Langendam M, Hairwassers D, Agoritsas T, Gijsen B, et al. Role of patient preferences in clinical practice guidelines: a multiple methods study using guidelines from oncology as a case. BMJ Open 2019; 9: e032483.
18. Armstrong MJ, Bloom JA. Patient involvement in guidelines is poor five years after institute of medicine standards: review of guideline methodologies. Res Involv Engagem 2017; 3: 19.
20. Lavis JN, Paulsen EJ, Oxman AD, Moynihan R. Evidence-informed health policy 2 - survey of organizations that support the use of research evidence. Implement Sci 2008; 3: 54.
21. Steinberg E, Greenfield S, Wolman DM, Mancher M, Graham R. Clinical practice guidelines we can trust. Washington (DC), National Academies Press. 2011.
22. Utens CM, van der Weijden T, Joore MA, Dirksen CD. The use of research evidence on patient preferences in pharmaceutical coverage decisions and clinical practice guideline development. BMC Health Serv Res 2014; 14: 540.
24. Sale JEM, Marwah A, Naeem F, Yu W, Meadows L. Evidence of patient beliefs, values, and preferences is not provided in osteoporosis clinical practice guidelines. Osteoporos Int 2019; 30: 1325-37.
25. Van der Wees PJ, Hendriks EJ, Custers JW, Burgers JS, Dekker J, de Bie RA. Comparison of international guideline programs to evaluate and update the Dutch program for clinical guideline development in physical therapy. BMC Health Serv Res 2007; 7: 191.
26. Utens CM, Dirksen CD, van der Weijden T, Joore MA. How to integrate research evidence on patient preferences in pharmaceutical coverage decisions and clinical practice guidelines. Health Policy 2016; 120: 120-8.
27. Kim C, Armstrong MJ, Berta WB, Gagliardi AR. How to identify, incorporate and report patient preferences in clinical guidelines: a scoping review. Health Expect 2020; 23: 1028-36.
28. Tringale M, Stephen G, Boylan AM, Heneghan C. Integrating patient values and preferences in healthcare: a systematic review of qualitative evidence. BMJ Open 2022; 12: e067268.
29. Muhlbacher AC, Sadler A, Juhnke C. Personalized diabetes management: what do patients with diabetes mellitus prefer? Eur J Health Econ 2021; 22: 425-43.
30. Zeng L, Helsingen LM, Bretthauer M, Agoritsas T, Vandvik PO, Mustafa RA, et al. A novel framework for incorporating patient values and preferences in making guideline recommendations. J Clin Epidemiol 2023; 161: 164-72.
31. Diaz Del Campo P, Gracia J, Blasco JA, Andradas E. A strategy for patient involvement in clinical practice guidelines: methodological approaches. BMJ Qual Saf 2011; 20: 779-84.
33. Bai F, Ling J, Esoimeme G, Yao L, Wang M, Huang J, et al. A systematic review of questionnaires about patient's values and preferences in clinical practice guidelines. Patient Prefer Adherence 2018; 12: 2309-23.
Patient values and preferences in guideline development
Fig. 1. Interpretation of recommendation strength within the GRADE framework.Strong recommendations are appropriate when expected benefits clearly outweigh harms and patient values and preferences are relatively consistent. Conditional recommendations are appropriate when benefits and harms are closely balanced and/or when values and preferences are expected to vary, signaling the need for shared decision-making. Examples shown are illustrative and not intended to be prescriptive: gastrectomy for T1 early gastric cancer (strong) and decision on adjuvant therapy (conditional).
Fig. 1.
Patient values and preferences in guideline development
Category
Method
Characteristics & Description
Key Outcome / Measure
Qualitative Methods
In-depth Interview
Explores individual experiences, values, and contextual backgrounds in detail. Useful for discovering novel value drivers.
Key concepts and value categories (Thematic analysis)
Focus Group Discussion (FGD)
Identifies shared opinions or conflicting views through group interaction. Often used for instrument development.
Group dynamics, consensus, and spectrum of perspectives
Quantitative Survey
Likert Scale
Measures level of agreement or importance using an ordinal ranking scale. Low cognitive burden and intuitive.
Mean scores, frequency distribution, response rates
Visual Analogue Scale (VAS)
Quantifies subjective value by asking respondents to mark their preference state on a continuous line (e.g., 0–100).
Mean score (0–100 scale), median values
Preference Elicitation
Discrete Choice Experiment (DCE)
Analyzes trade-offs by requiring respondents to choose between hypothetical scenarios defined by varying attributes and levels.
Part-worth utility, relative importance, marginal rates of substitution
Best-Worst Scaling (BWS)
Measures preference intensity by asking respondents to select the "best" (most important) and "worst" (least important) items.
Preference scores, relative importance rankings
Utility Measurement
Standard Gamble (SG)
Measures health state utility based on decision-making under uncertainty (risk).
Utility values (0–1), basis for quality-adjusted life year (QALY) calculation
Time Trade-Off (TTO)
Measures utility by determining the indifference point between a duration in a specific health state and a shorter duration in perfect health.
Utility values, weights for quality-adjusted life year (QALY) calculation
Table 1. Types and Characteristics of Patient Values and Preferences Research Methods