This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Post-thyroidectomy hypocalcemia is the most frequent complication after total thyroidectomy. Preoperative vitamin D deficiency has been suggested as a potential risk factor, but inconsistencies exist in the literature, possibly related to methodological differences. To evaluate whether study design and risk of bias influence the association between preoperative vitamin D deficiency and postoperative hypocalcemia in patients undergoing total thyroidectomy.
Methods
This is a secondary analysis of a previously conducted systematic review. We included observational studies evaluating the association between preoperative vitamin D levels and postoperative hypocalcemia. Methodological quality was assessed using the QUIPS tool. Subgroup analyses were performed based on study design (prospective vs. retrospective) and overall risk of bias (high vs. low/moderate).
Results
Twenty-eight studies comprising 4994 patients were included. Nineteen studies had a prospective design. Both prospective and retrospective studies showed an association between vitamin D deficiency and hypocalcemia; however, the effect size was lower in prospective studies (OR 1.95; 95% CI 1.28-2.97) compared to retrospective ones (OR 2.18; 95% CI 1.02-4.7). Studies with high risk of bias showed a significant association (OR 2.55; 95% CI 1.4-3.6), while those with low/moderate risk did not (OR 1.71; 95% CI 0.96-3.06).
Conclusion
Study design and methodological quality influence the reported association between vitamin D deficiency and postoperative hypocalcemia. These findings suggest caution when recommending preoperative vitamin D supplementation based solely on observational data.
Thyroidectomy is the most frequently performed endocrine surgical procedure in the world [1]. Almost all of total thyroidectomy complications occur as a result of postoperative hypocalcemia [2]. Symptomatic temporary hypocalcemia is usually mild and transient, however permanent hypocalcemia could occur in almost 16% of patients [3], and is associated with prolonged hospital stay, reduced quality of life, and an increased use of resources. Advanced age, female sex, hyperthyroidism, inadvertent resection of the parathyroid glands, and low preoperative vitamin D levels have been suggested as risk factors for the development of postoperative hypoparathyroidism [4].
Vitamin D deficiency is frequent and asymptomatic because of a mix of poor dietary intake of Vitamin D-rich foods, malabsorption and inadequate exposure to natural sunshine. Individuals with vitamin D deficiency are more likely to develop hypocalcemia following thyroidectomy and several researchers have suggested preventive calcitriol and calcium treatment before surgery [5]. In a recent systematic review [6], we demonstrated that there is a threshold effect in the classification of vitamin D deficiency, which influences its association with postoperative hypocalcemia. Other factors to explore are differences in study design and methodological quality. There is considerable evidence in the literature that retrospective and observational studies inform a greater association between causal variables and outcomes than prospective and experimental studies [7]. Besides, studies having a high risk of bias are more likely to provide statistically significant results than those with a low risk of bias [8]. This support investigating this aspect as a possible moderator of the relationship between vitamin D deficiency and postoperative hypocalcemia.
Aims
The purpose of this study is to identify that study design characteristics are moderators in the causal association between preoperative vitamin D deficiency and the incidence of biochemical hypocalcemia in patients having total thyroidectomy. The present analysis builds upon a previously published systematic review but addresses specific methodological dimensions, such as study design, risk of bias, and the distribution of statistically significant outcomes, that were not prespecified or explored in the original protocol.
Methods and Material
This is a study that does not use patient data, and no evaluation by the research ethics committee was necessary. The methodology for this study was detailed in a previous publication, which examined the threshold effect in identifying vitamin D deficiency and its impact on the occurrence of hypocalcemia [6]. A systematic review of the literature was conducted following the Cochrane Collaboration and PRISMA methodology guidelines. Studies that described the preoperative measurement of vitamin D in adult patients undergoing total thyroidectomy and investigated its association with the development of postoperative hypocalcemia were included. There were no limitations on the publishing date, language, design, number of patients studied, or type of publication. Vitamin D levels were measured before surgery, as well as biochemical post-operative hypocalcemia using the study-specific method. The literature search included Medline, EMBASE, Google Scholar and LILACS databases, Finally, the selected studies were evaluated, and those that met the inclusion criteria were included. Data about methodological characteristics of the studies and the clinical characteristics of the patients were collected. The Quality In Prognosis Studies (QUIPS) instrument was used to assess the methodological quality of the studies. The RevMan 5.3 software was used (Review Manager (RevMan) [Computer program]. The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2014). For dichotomous outcomes, results were expressed as odds ratio (OR) with 95% confidence intervals using a random effects model. A subgroup analysis based on study design (prospective or retrospective), global methodological quality and domains from the QUIPS instrument was made to investigate the effect.
Statistical heterogeneity was estimated using the Higgins I2 statistic. The results of the intervention effects are illustrated with a forest plot graph.
Results
After literature review 28 studies published between 2007 and 2022 were included [9-11,2,12-18,3,19-34]. The overall analysis included 4994 patients, categorized into two groups: 2256 with sufficient vitamin D levels and 2738 with vitamin D deficiency.
Study design
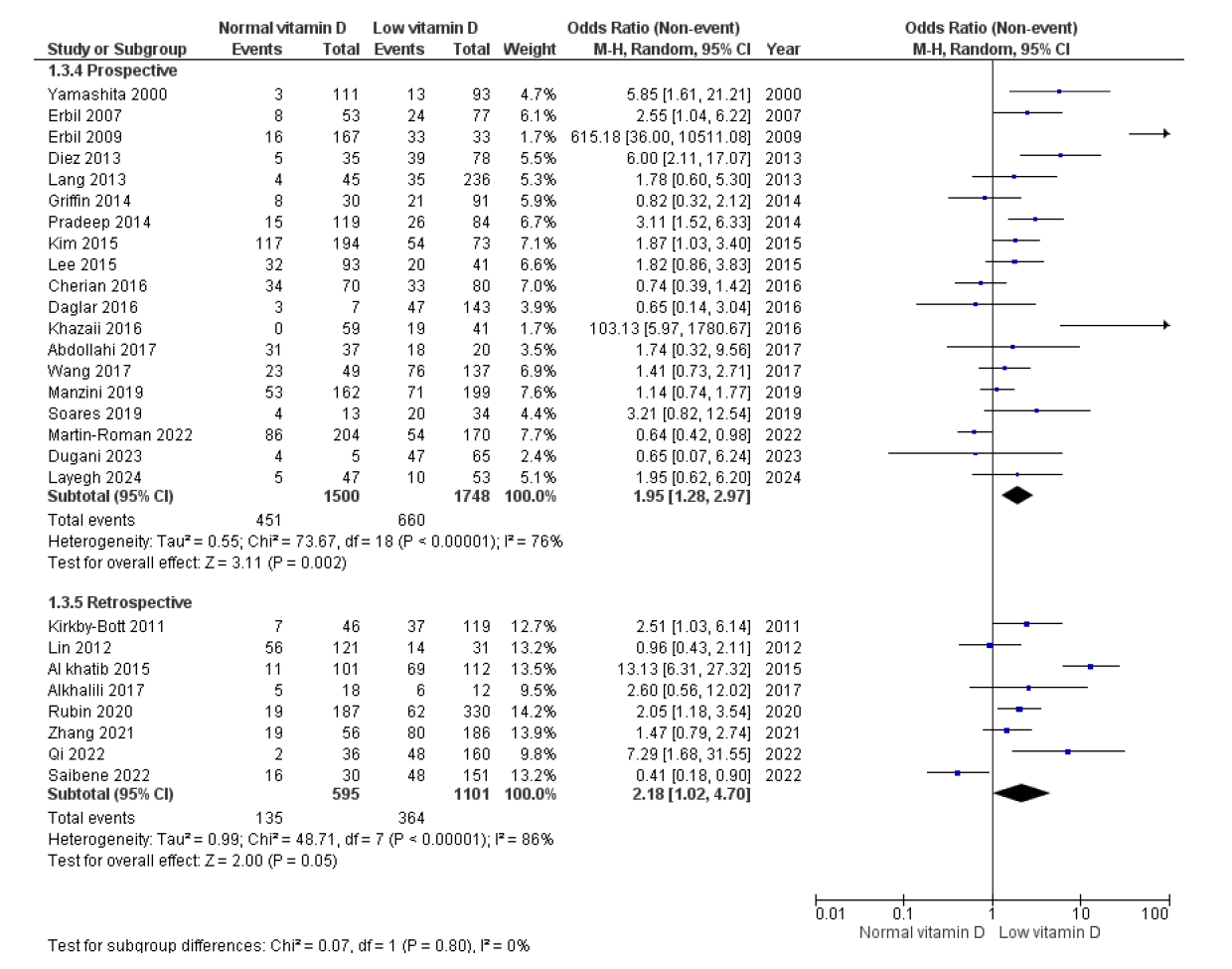
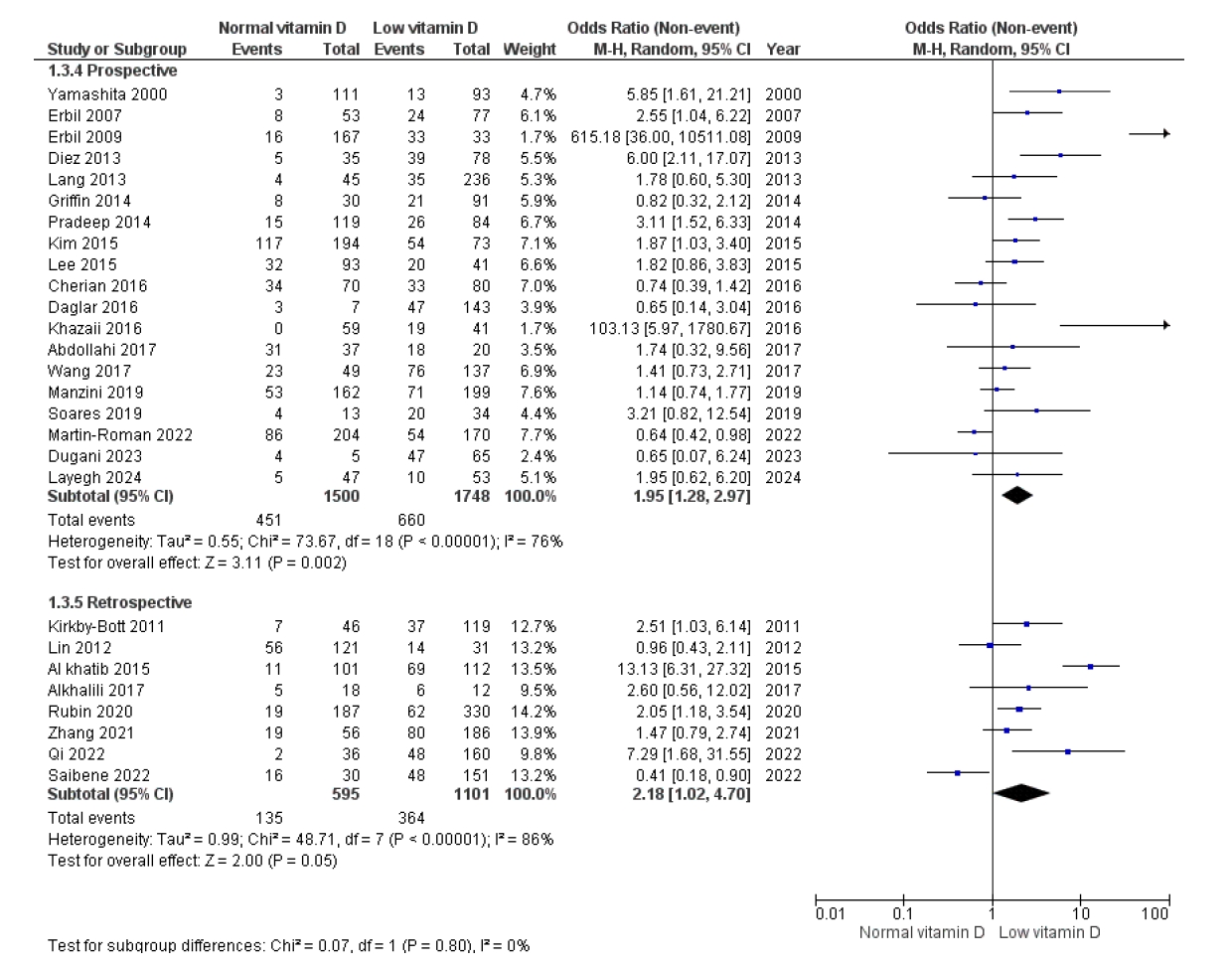
Nineteen studies (67%) had a prospective design [9,2,12-18,3,20-22,25-27,31-33], whereas the remainder were retrospective. Both types of designs found an association between vitamin D deficiency and postoperative hypocalcemia, but the magnitude of the effect was smaller in prospective studies (OR = 1.95 (1.28-2.97) vs. retrospective studies (OR = 2.18 (1.02-4.7)), though this was not statistically significant (p for subgroup differences = 0.8). (Figure 1).
Risk of bias
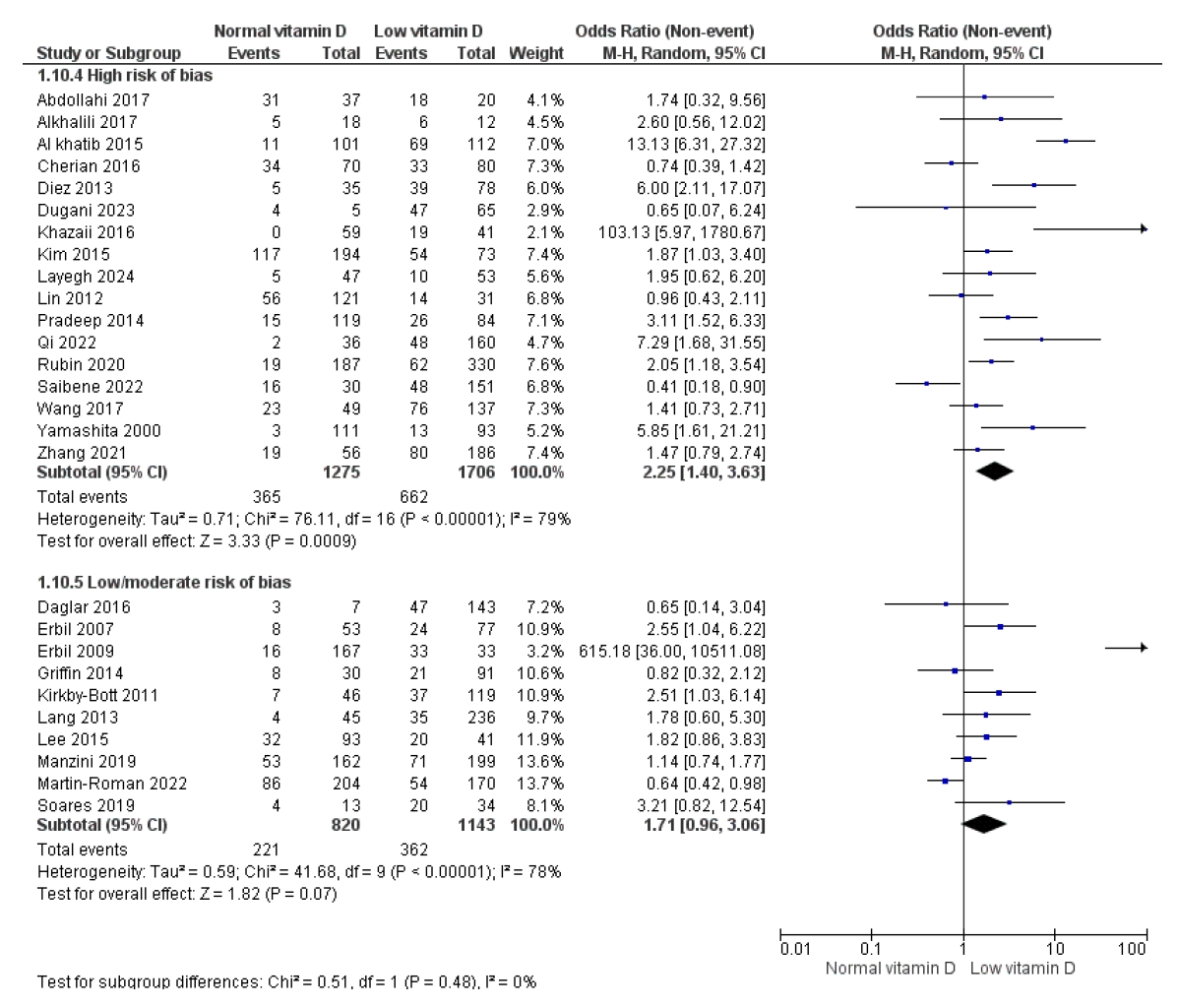
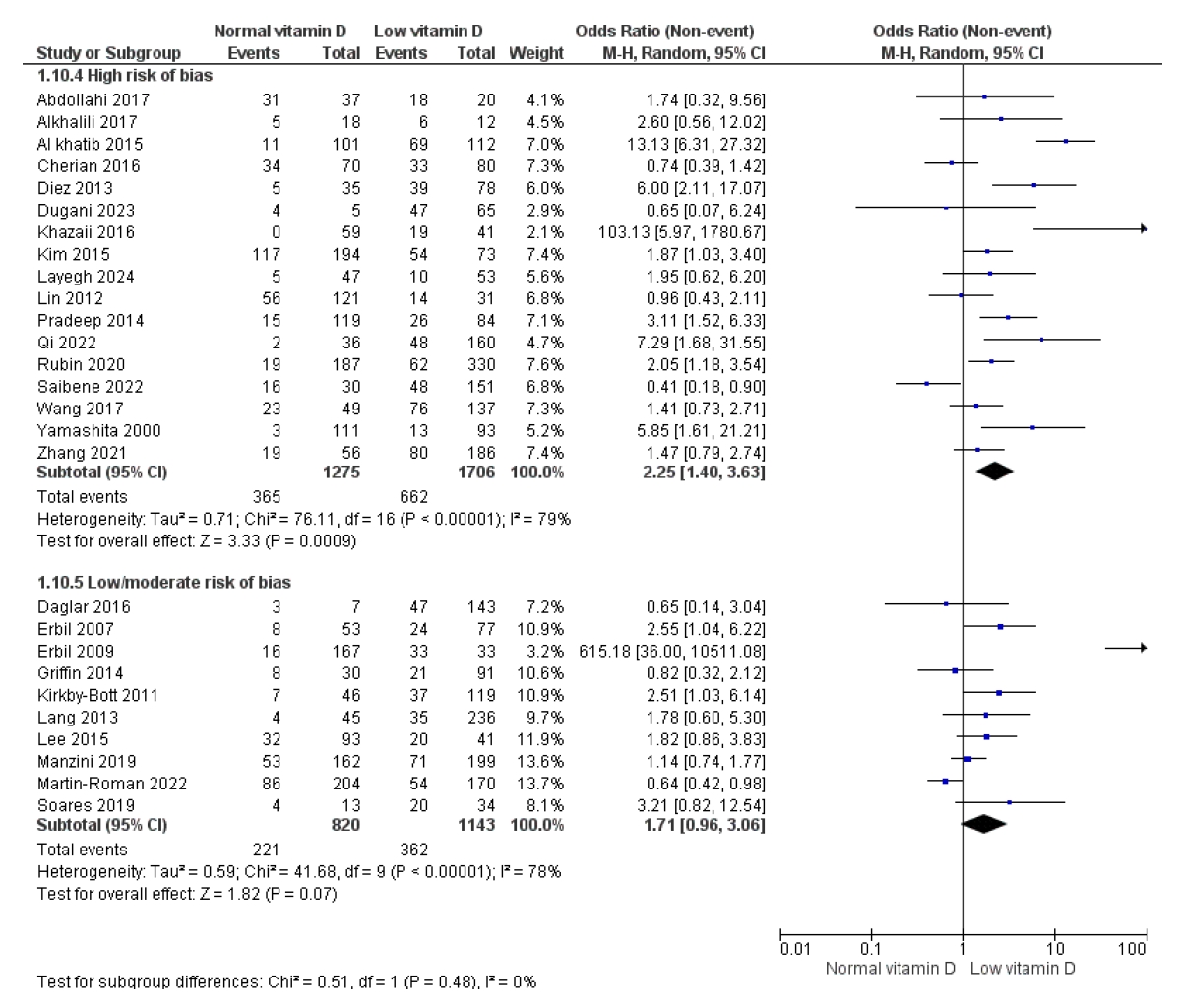
The overall risk of bias of the studies included was suboptimal, with 17 (60%) falling into the high risk of bias group [9-11,2,13,18,3,23,27-30,32-34,14,21]. Studies with a high risk of bias found an association between vitamin D deficiency and postoperative hypocalcemia (OR 2.55 (95% CI 1.40-3.63), but those with a moderate or low risk showed no such association (OR 1.71 (95% CI 0.96-3.06), although this difference was not statistically significant (p for group comparison =0.48) (Figure 2).
Twenty-five percent of the studies were judged to have a high risk of bias in the study participation domain, 36% in the study attrition, 46% in the study confounding and 29% in the statistical analysis domain (Table 1).
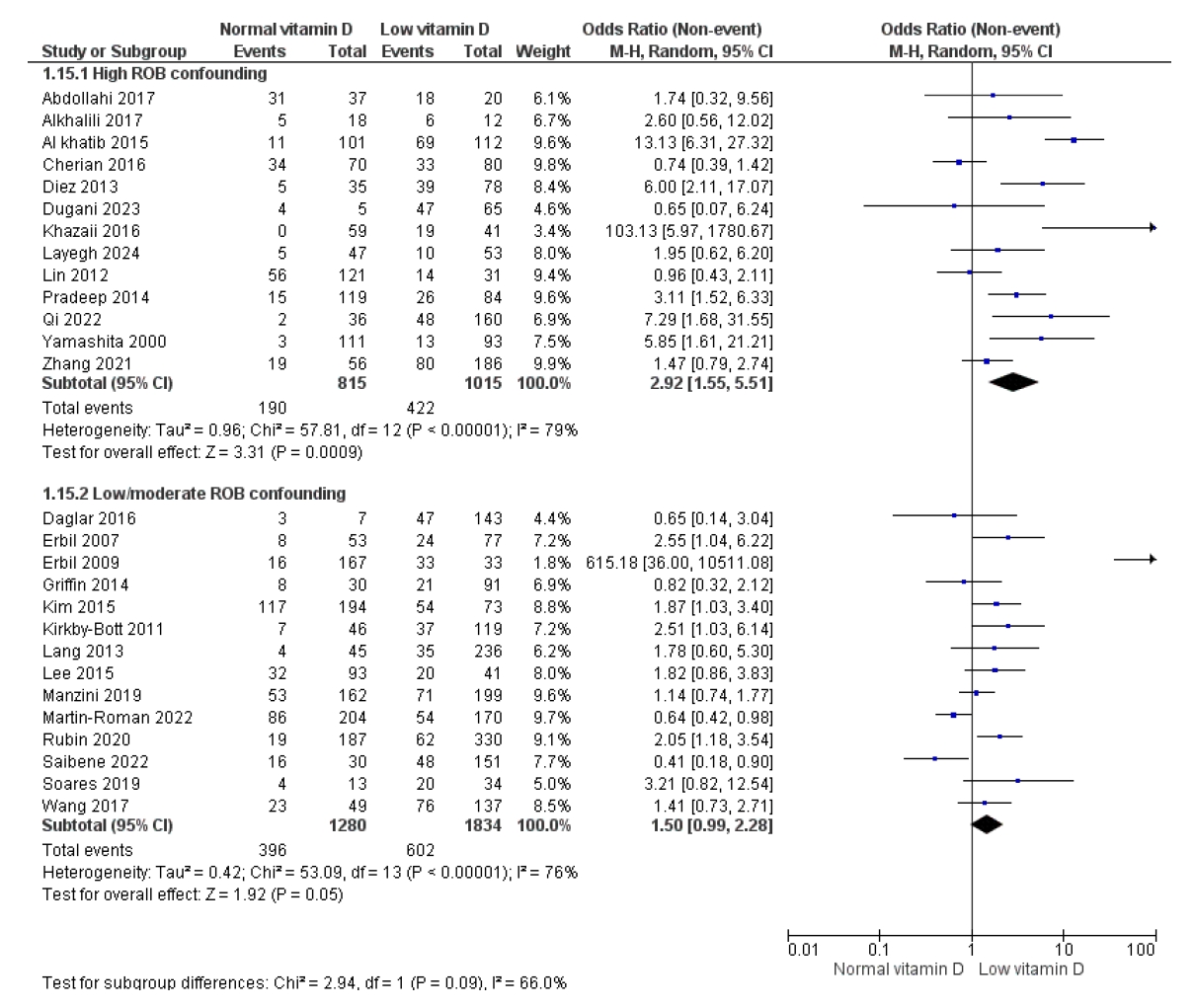
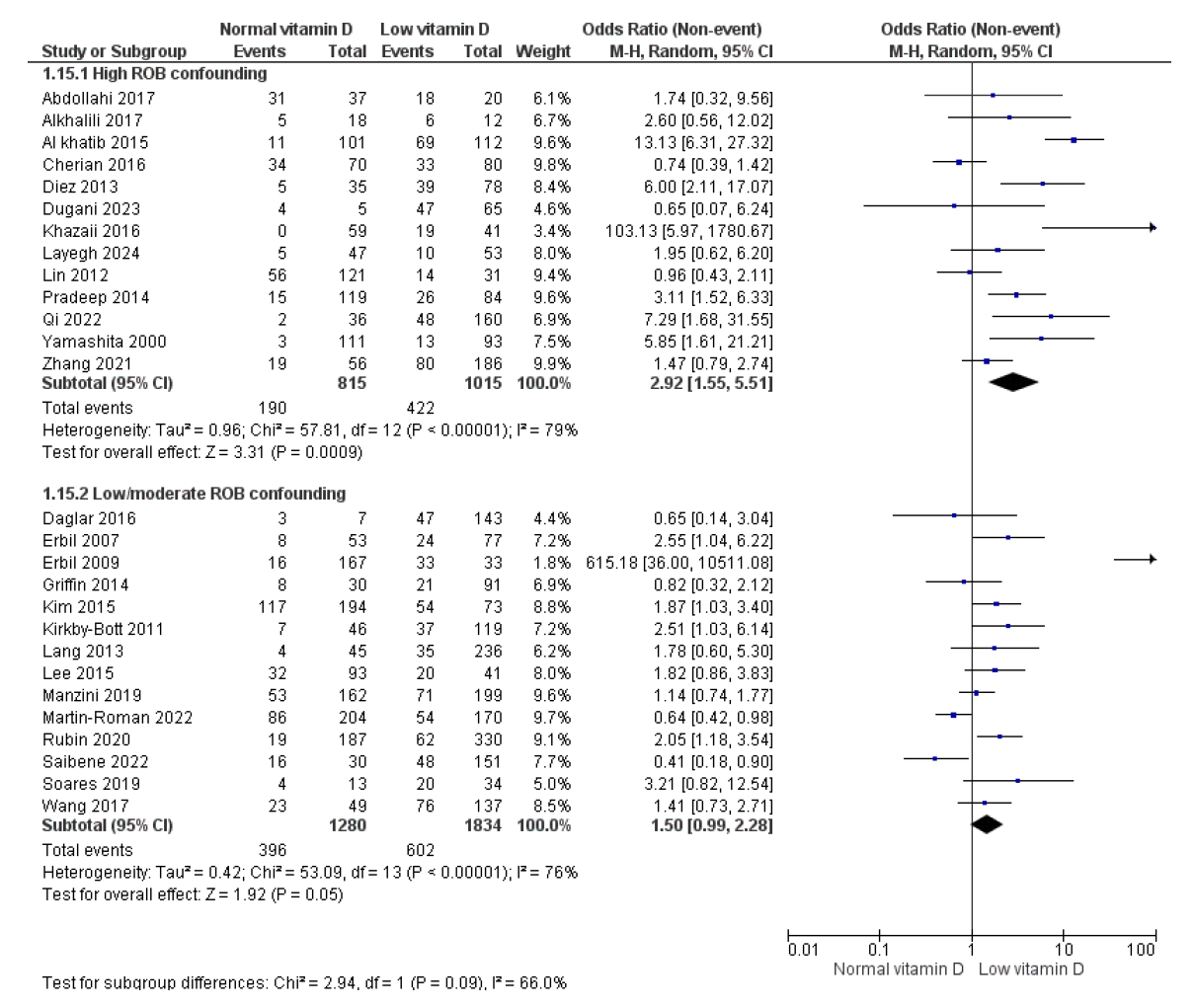
The confounding domain revealed the most frequent flaws. There were significant shortcomings in the identification, definition, and measurement of potential clinical confounders (need for neck dissection) and co-interventions (use of autologous parathyroid transplantation, routine postoperative calcium administration), as well as the methods employed to adjust for the association. This is also relevant to statistical analysis and reporting, as the statistical studies did not apply adjustment models to test the causal association's independence. Studies with a confounding domain assessed as low/moderate risk of bias reported no link between vitamin D deficiency and hypocalcemia (OR 1.50 (95% CI 0.99-2.28) versus 2.92 (95% CI 1.55-5.51) (Figure 3).
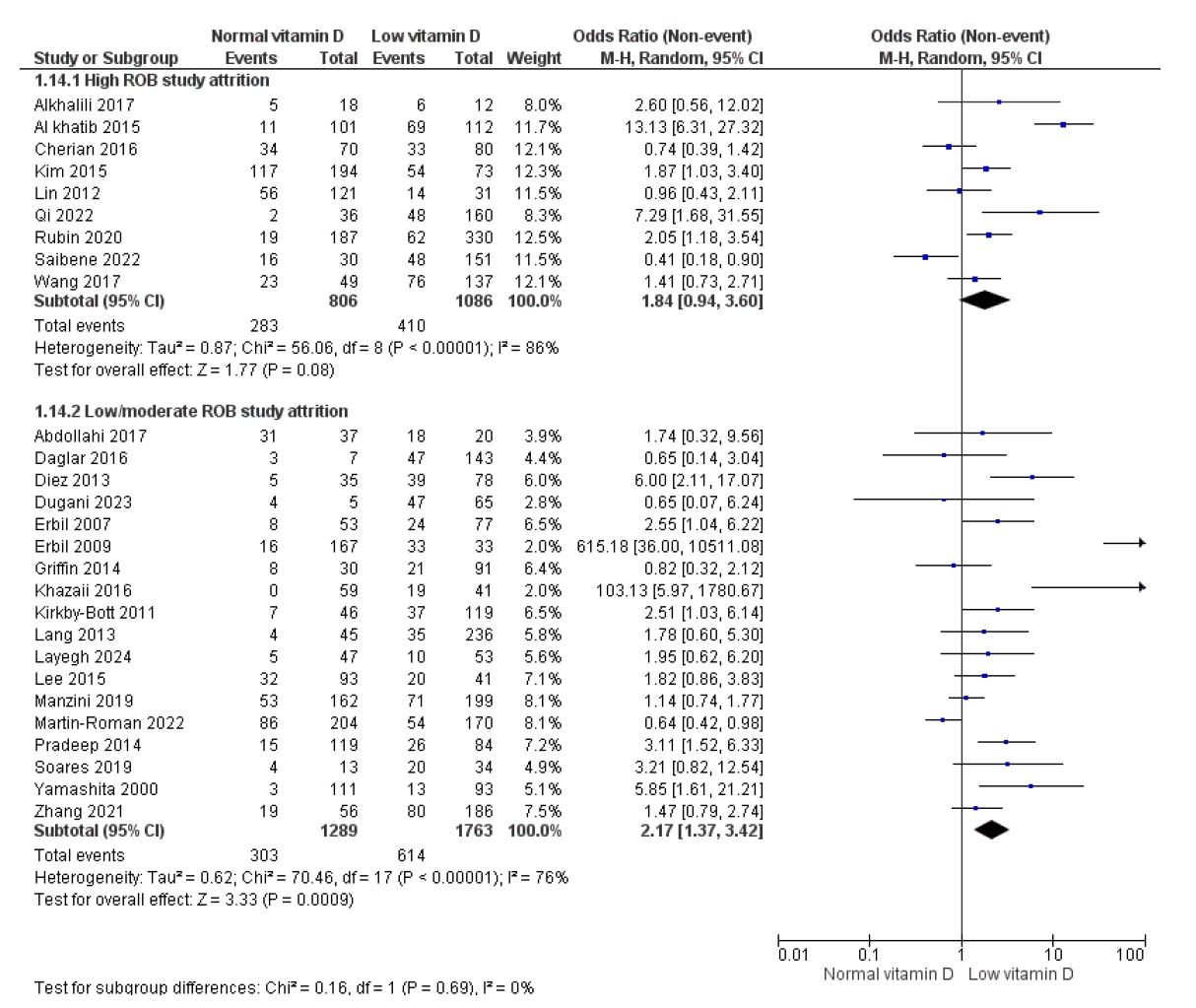
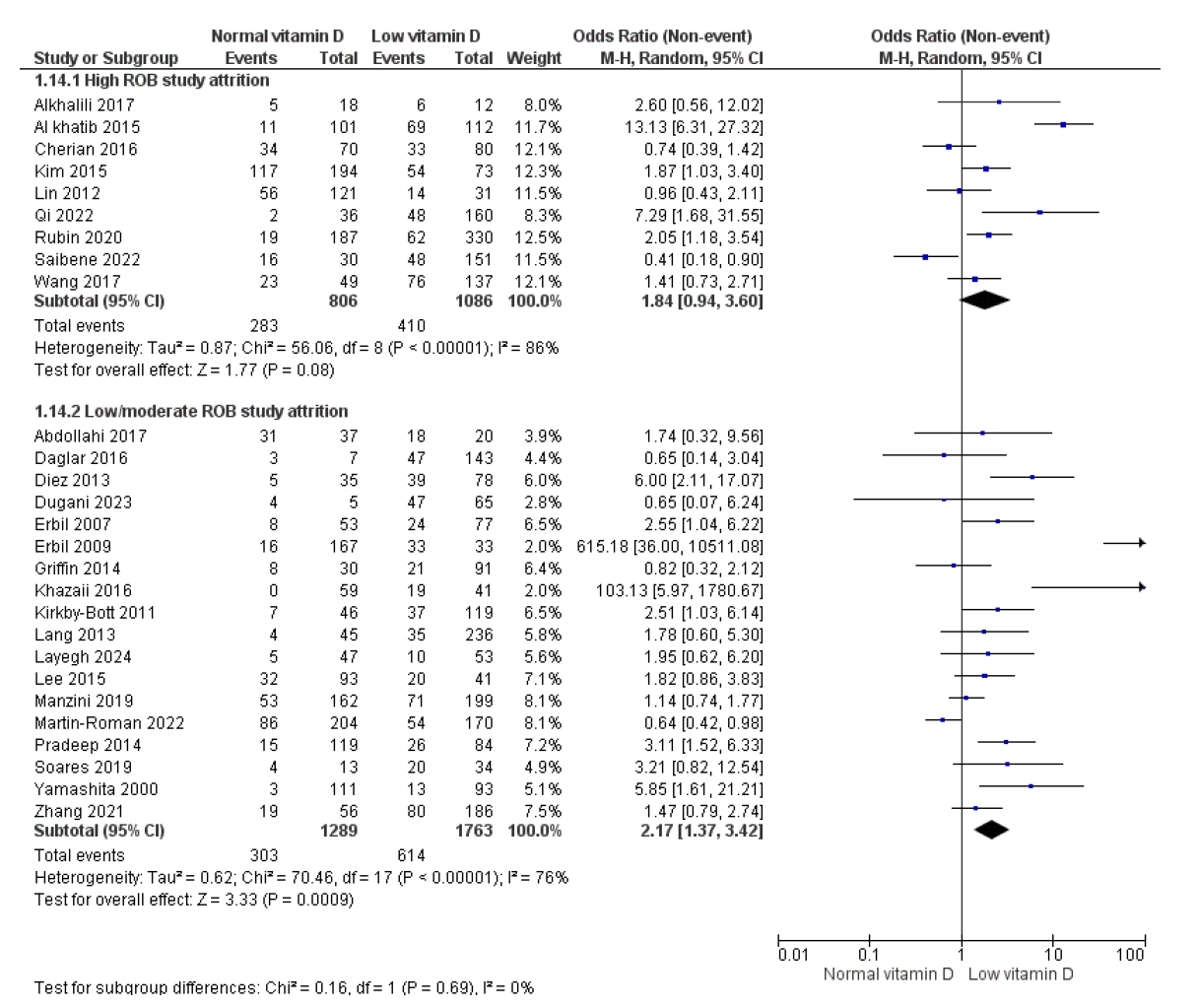
The attrition study domain major flaws were an inadequate description of the response rate, the lack of attempts to acquire information from patients who dropped out of the trial, and the description of the causes and characteristics of these patients. Studies with a low/moderate risk of bias in the study attrition domain demonstrated an association between hypocalcemia and vitamin D deficiency (OR 2.17 [95% CI 1.37–3.42] vs 1.84 [95% CI 0.94–3.60]) (Figure 4).
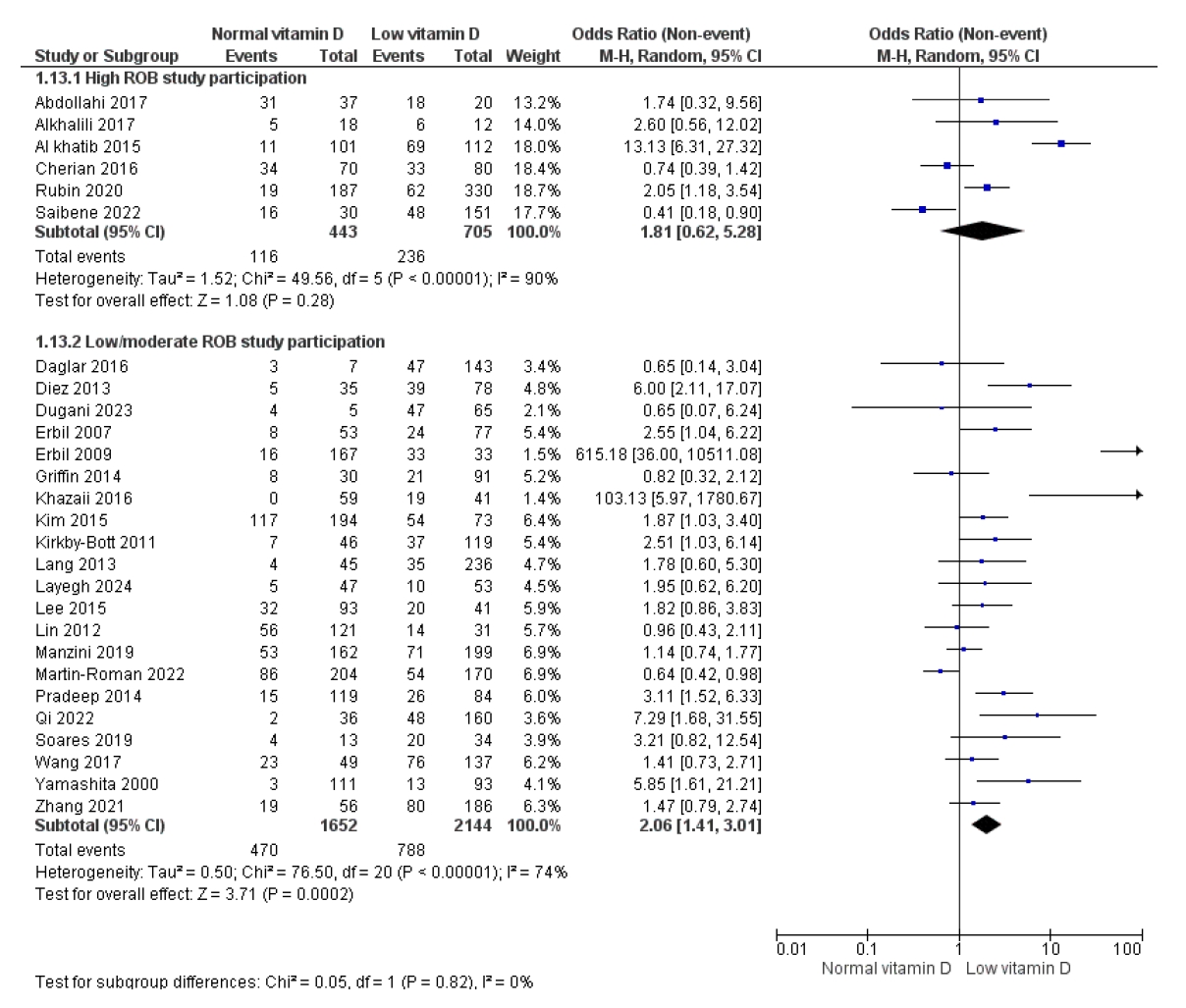
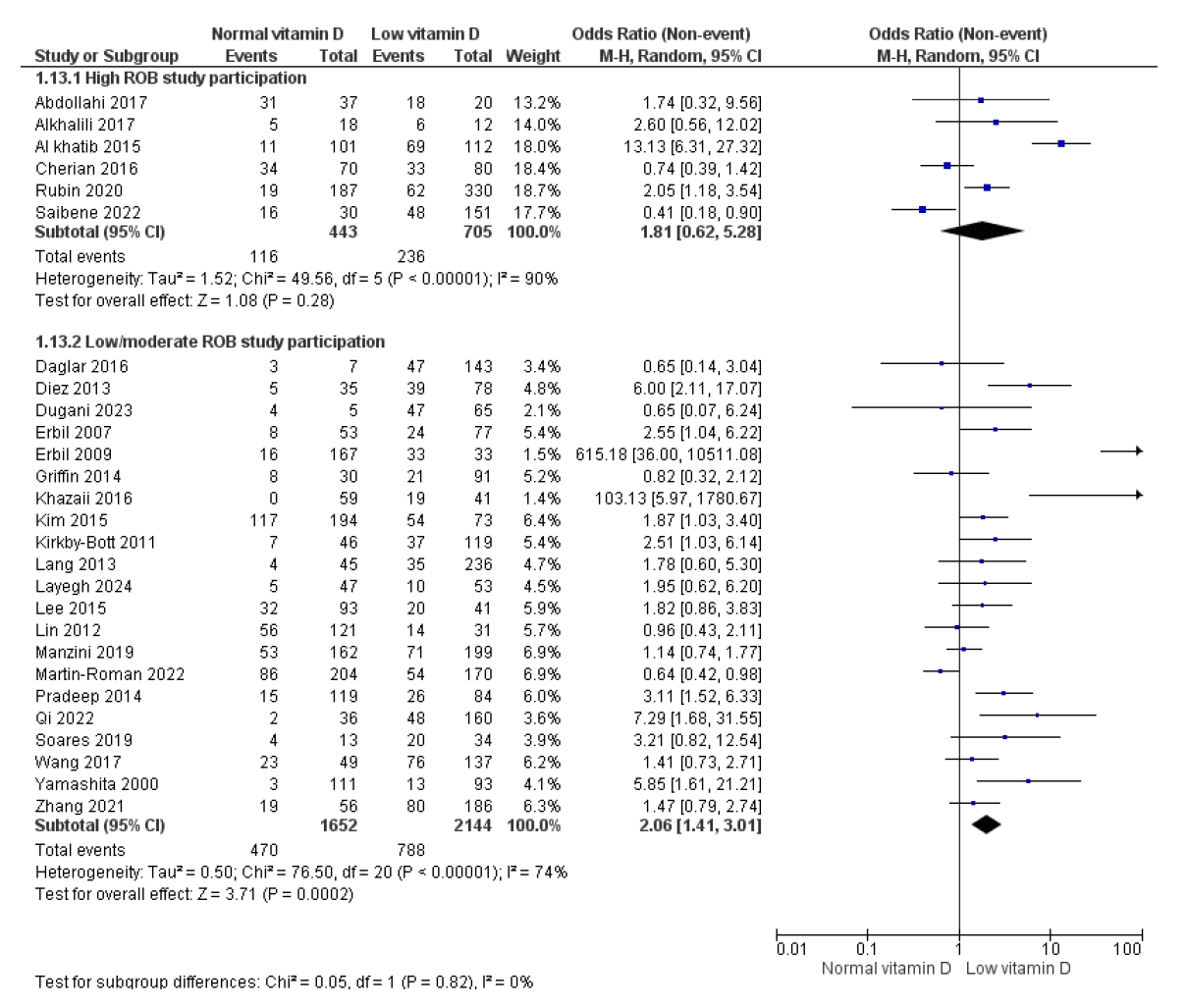
Finally, in terms of selection bias, the most significant weaknesses were an inadequate description of the method used to identify the population, a lack of definition of specific inclusion and exclusion criteria, and a lack of information about eligible individuals' participation. Studies categorized into a low/moderate risk of bias participation domain showed an association between vitamin D deficiency and hypocalcemia (OR 2.06 [95% CI 1.41–3.01] compared to 1.81 [95% CI 0.62–5.28]) (Figure 5).
Discussion
We previously demonstrated the existence and impact of the threshold effect in defining vitamin D deficiency on its association with postoperative hypocalcemia [6], where a lower threshold corresponds to an increased incidence of hypocalcemia. Nonetheless, there are other aspects in the original studies, which have not been well assessed and may influence the strength of this association [5,11,17,35].
The literature provides information about the overestimation of association estimates in observational research compared to randomized clinical trials. Nonetheless, in causality research, employing a randomized approach is unfeasible due to clinical or ethical considerations. Consequently, other components of observational research design are pertinent, including direction (cohort or case-control studies), temporality (prospective vs retrospective), and risk of bias assessment. Cohort studies are superior to case-control studies due to the potential for improved data quality and lower susceptibility to biases, such as recall bias. This systematic review predominantly includes cohort studies, which improves the reliability of the results relative to other observational designs.
The relationship between the prospective or retrospective design of cohort studies and the risk of bias is among the most extensively examined methodological issues [36]. Prospective cohort studies are thought to be of greater quality than retrospective studies because they provide more exact control over the collection of causal variables, co-interventions, and outcomes while also ensuring the temporal link between exposure and outcome. However, this comes at the expense of a longer research time and the inability to collect an adequate number of subjects when outcomes are extremely infrequent [36]. Nonetheless, elements such as variability in the definitions of prospective versus retrospective studies and adequate compliance with additional factors, including the thorough collection of primary data, pertinent confounding variables, and appropriate statistical adjustments, indicate that the study design alone does not ensure high methodological quality [37]. Although this study included 67% of retrospective cohorts, it found that the design was not a statistically significant methodological factor in the relationship between vitamin D insufficiency and postoperative hypocalcemia. However, prospective studies had a lower effect size (OR 1.95 vs 2.18). This data suggests that while there is an association between vitamin D deficiency and hypocalcemia, its extent may be influenced by design considerations, indicating that future research should account for this condition to mitigate the possibility of overestimation.
The overall assessment of the risk of bias is an important component in the critical interpretation of observational study results [8]. A high risk of bias compromises the study's internal validity by adding distortions that might change the magnitude, direction, or even the presence of an association between exposure and result, establish false associations, or mask true effects. Even when the results are statistically significant, the study's ability to establish accurate causal conclusions is limited by the significant risk of bias.
Nineteen studies included in this systematic review were identified as having a high risk of bias, and it was possible to show that the association between vitamin D deficiency and postoperative hypocalcemia varies between studies with different methodological quality. This finding jeopardizes the established association between these two factors.
A more comprehensive review of the QUIPS domains that assessed the risk of bias provided some reasons. First, the most common weakness in primary research was adjustment for confounding factors. This bias happens when a variable has an association to both the exposure and the outcome without being part of the causal pathway, resulting in inaccurate estimations of the real effect. These deficiencies threaten the validity of impact estimates [38]. Gao et al. [39], examined 162 observational studies published between 2018 and 2023 and discovered that only 6.2% adopted the suggested approach of confounder correction for each exposure-outcome association. In this review, studies that did not adequately adjust for clinical factors reported significantly stronger associations between vitamin D deficiency and hypocalcemia (OR 2.92; 95% CI: 1.55–5.51) than those with a low or moderate risk of bias in the confounding domain, where the association was inconclusive (OR 1.50; 95% CI: 0.99–2.28).
This study also found flaws in both selection and attrition bias [40]. In terms of selection bias, typical issues included a lack of a clear description of the population identification process, poorly defined inclusion and exclusion criteria, and insufficient information on eligible persons' participation. These methodological flaws could threaten the study's representativeness and provide erroneous associations if the inclusion probabilities are related to exposure or outcome. Studies with a low or moderate risk of bias in this area found a stronger link between vitamin D insufficiency and hypocalcemia (OR 2.06; 95% CI: 1.41-3.01) than those with a high risk (OR 1.81; 95% CI: 0.62-5.28). On the other hand, attrition bias was characterized by an inadequate description of the response rate, the absence of attempts to reach patients who fell out of follow-up, and a lack of information on the causes and characteristics of these losses. This omission may generate bias if patients who do not finish the research differ significantly from those who do. In fact, studies with a lower risk of attrition bias found a stronger association between hypocalcemia and vitamin D deficiency (OR 2.17; 95% CI: 1.37-3.42) than those with higher risk (OR 1.84; 95% CI: 0.94-3.60) [41]. The findings of this study [6] indicate flaws in fulfilling some of requirements as size of the effect, specificity and experimental proof [5] and call into question the causal hypothesis between vitamin D deficiency with post-thyroidectomy hypocalcemia. They may also explain why trials evaluating preoperative prophylactic administration of vitamin D to prevent postoperative hypocalcemia have reached divergent conclusions [42]. Finally, it is a source of information that can be utilized to develop new research that addresses the flaws of existing ones.
The current study has various limitations due to its design as a secondary analysis of a systematic review, as it was not originally designed with the current research issue in mind. However, the primary review followed current recommendations for this type of study. Potential interactions between the domains used to assess risk of bias were also not investigated, making it impossible to determine which of these domains is more prominent.
Conclusion
This analysis demonstrates that the methodological quality and design of observational studies have an important influence on the magnitude of the established association between vitamin D insufficiency and postoperative hypocalcemia. Although a tendency toward a positive association is evident, it is more prominent in studies with a high risk of bias and retrospective designs. These findings stress the importance of caution when interpreting existing results in conjunction with development of new research with prospective designs, confounding control, and a comprehensive assessment of bias risk. Clinical decisions for vitamin D supplementation in the surgical setting should be based on individual clinical judgment rather than a presumption of causality.
Forrest plot comparing biochemical hypocalcemia and Vitamin D deficiency according to study design.
Fig. 2.
Forrest plot comparing biochemical hypocalcemia and Vitamin D deficiency according to study risk of bias global evaluation.
Fig. 3.
Forrest plot comparing biochemical hypocalcemia and Vitamin D deficiency according to study risk of bias domain confusion.
Fig. 4.
Forrest plot comparing biochemical hypocalcemia and Vitamin D deficiency according to study risk of bias domain attrition.
Fig. 5.
Forrest plot comparing biochemical hypocalcemia and Vitamin D deficiency according to study risk of bias domain participation.
Table 1.
Evaluation of Risk of Bias Using the Domains of QUIPS Tool
Study
1. Study Participation
2. Study Attrition
3. Prognostic Factor Measurement
4. Outcome Measurement
5. Study Confounding
6. Statistical Analysis and Reporting
Abdollahi
High
Low
High
Low
High
High
Alkhalili
High
High
Low
Low
High
High
Alkhatib
High
High
Low
Low
High
Moderate
Cherian
High
High
Low
Low
High
Moderate
Daglar
Low
Low
Low
Low
Moderate
Low
Diez
Moderate
Low
Low
Low
High
Low
Dugani
Low
Low
Low
Low
High
High
Erbil 2007
Low
Low
Low
Low
Moderate
Low
Erbil 2009
Low
Low
Low
Low
Moderate
Low
Griffin
Low
Low
Low
Low
Moderate
Low
Khazaii
Moderate
Moderate
Moderate
Low
High
High
Kim
Low
High
Low
Low
Moderate
Low
Kirbi
Moderate
Moderate
Low
Low
Moderate
Moderate
Lang
Low
Low
Low
Low
Low
Low
Layegh
Low
Low
Low
Low
High
High
Lee
Low
Low
Low
Low
Moderate
Low
Lin
Moderate
High
Low
Low
Moderate
Low
Malikarjuna
High
High
Low
Low
High
High
Manzini
Low
Low
Low
Low
Low
Low
Martin
Low
Low
Low
Low
Low
Low
Pradeep
Low
Low
Low
Low
High
High
Qi
Moderate
High
Low
Low
High
Moderate
Rubin
High
High
Low
Low
Moderate
Low
Saibene
High
High
Low
Low
Moderate
Low
Soares
Low
Low
Low
Low
Low
Low
Wang
Moderate
High
Low
Low
Moderate
Low
Yamashita
Low
Low
Low
Low
High
High
Zhang
Low
Low
Low
Low
High
Moderate
Number of high risk of bias studies
7
10
1
0
13
8
%
25%
36%
4%
0%
46%
29%
References
1. Omi Y, Hasegawa Y, Takami H, Ito Y, Miyauchi A, Sugitani I, et al. Trends in thyroid surgery in Japan from 2014 to 2023: report on the National Clinical Database. Surg Today. 2025.
2. Cherian AJ, Gowri M, Ramakant P, Mishra A, Agarwal G, Agarwal A. The role of vitamin D in post-thyroidectomy hypocalcemia: still an enigma. Surgery 2016; 159: 532-8.
3. Kim WW, Kim JS, Hur SM, Kim SH, Lee SK, Choe JH, et al. Is preoperative vitamin D deficiency a risk factor for postoperative symptomatic hypocalcemia in thyroid cancer patients undergoing total thyroidectomy plus central compartment neck dissection. Thyroid 2015; 25: 911-8.
5. Vaitsi KD, Anagnostis P, Veneti S, Artzouchaltzi AM, Goulis DG, Kita M, et al. Preoperative vitamin D deficiency is a risk factor for postthyroidectomy hypoparathyroidism: a systematic review and meta-analysis of observational studies. J Clin Endocrinol Metab 2021; 106: 1209-24.
6. Lopera K, Sanabria A. Threshold-dependent risk of postoperative hypocalcemia in vitamin D-deficient patients undergoing total thyroidectomy: a meta-analysis. Surgery 2025; 182: 109333.
8. Sterne J, et al. Chapter 25: Assessing risk of bias in a non-randomized study. In: Higgins J, Thomas J, Chandler J, , editors. Cochrane handbook for systematic reviews of interventions version 6.5. London, Cochrane. 2024.
9. Abdollahi A, et al. Is there any relationship between serum level of vitamin D and postoperative hypocalcemia after total thyroidectomy. Biomed Pharmacol J 2017;
10. Al-Khatib T, Althubaiti A, Althobaiti A, Alzahrani A, Alzahrani M, Alghamdi A, et al. Severe vitamin D deficiency: a significant predictor of early hypocalcemia after total thyroidectomy. Otolaryngol Head Neck Surg 2015; 152: 424-31.
11. Alkhalili E, Al-Ali S, Al-Omari A, Alsharari A, Alenezi K, Alshammari F, et al. Does pre-operative vitamin d deficiency predict postoperative hypocalcemia after thyroidectomy. Endocr Pract 2017; 23: 5-9.
12. Dağlar G, Karaköse M, Tutal E, Çalışkan K, Deyneli O, Yıldız BO, et al. Is there a relationship between vitamin d status and hypocalcemia after total thyroidectomy. Acta Endocrinol (Buchar) 2016; 12: 291-6.
13. Díez M, Vera C, Ratia T, Diego L, Mendoza F, Guillamot P, et al. Effect of vitamin D deficiency on hypocalcaemia after total thyroidectomy due to benign goitre. Cir Esp 2013; 91: 250-6.
14. Dugani P, Singh S, Kaur R, Sharma A, Bansal A, Kaur M, et al. Serum parathyroid hormone and vitamin D levels as predictors of hypocalcemia after total/near total thyroidectomy. Indian J Otolaryngol Head Neck Surg 2023; 75: 1502-10.
15. Erbil Y, Barbaros U, Temel B, Turkoglu U, Işsever H, Bozbora A, et al. The impact of age, vitamin D(3) level, and incidental parathyroidectomy on postoperative hypocalcemia after total or near total thyroidectomy. Am J Surg 2009; 197: 439-46.
16. Erbil Y, Barbaros U, Işsever H, Ozarmağan S, Tezelman S, Ozbaş S, et al. Predictive value of age and serum parathormone and vitamin d3 levels for postoperative hypocalcemia after total thyroidectomy for nontoxic multinodular goiter. Arch Surg 2007; 142: 1182-7.
17. Griffin TP, Murphy MS, Sheahan P, Quinn EM, O’Leary DP, McAnena OJ, et al. Vitamin D and risk of postoperative hypocalcemia after total thyroidectomy. JAMA Otolaryngol Head Neck Surg 2014; 140: 346-51.
18. Khazaii A, Ramazani M. Post-thyroidectomy hypocalcemia and pre-operative vitamin D levels. Acad J Surg 2016; 3: 54-7.
19. Kirkby-Bott J, Markogiannakis H, Skandarajah A, Cowan M, Fleming B, Palazzo F, et al. Preoperative vitamin D deficiency predicts postoperative hypocalcemia after total thyroidectomy. World J Surg 2011; 35: 324-30.
20. Lang BH, Wong KP, Cheung CY, Wan KY, Lo CY. Does preoperative 25-hydroxyvitamin D status significantly affect the calcium kinetics after total thyroidectomy. World J Surg 2013; 37: 1592-8.
21. Layegh P, Sajjadi ZS, V Mostaan L, Mohebbi M, Kabiri M, Yaghoubi MA. Preoperative vitamin D status and post-total thyroidectomy hypocalcemia. Iran J Otorhinolaryngol 2024; 36: 343-8.
22. Lee GH, Ku YH, Kim HI, Lee MC, Kim MJ. Vitamin D level is not a predictor of hypocalcemia after total thyroidectomy. Langenbecks Arch Surg 2015; 400: 617-22.
23. Lin Y, Ross HL, Raeburn CD, DeWitt PE, Albuja-Cruz M, Jones EL, et al. Vitamin D deficiency does not increase the rate of postoperative hypocalcemia after thyroidectomy. Am J Surg 2012; 204: 888-93. discussion 893-4.
24. Mallikarjuna N, et al. Correlation of pre-operative vitamin D3 levels with post-operative hypocalcemia in patients undergoing total thyroidectomy. Int Surg J 2020; 7: 128-32.
27. Pradeep PV, Ramalingam K. Postoperative PTH measurement is not a reliable predictor for hypocalcemia after total thyroidectomy in vitamin D deficiency: prospective study of 203 cases. World J Surg 2014; 38: 564-7.
28. Qi Y, Chai J, Zhang L, Chen Y. Preoperative vitamin D level is significantly associated with hypocalcemia after total thyroidectomy. BMC Musculoskelet Disord 2022; 23: 1118.
29. Rubin SJ, Park JH, Pearce EN, Holick MF, McAneny D, Noordzij JP. Vitamin D status as a predictor of postoperative hypocalcemia after thyroidectomy. Otolaryngol Head Neck Surg 2020; 163: 501-7.
30. Saibene AM, Rosso C, Felisati G, Pipolo C, De Leo S, Lozza P, et al. Can preoperative 25-hydroxyvitamin D levels predict transient hypocalcemia after total thyroidectomy. Updates Surg 2022; 74: 309-16.
32. Wang X, Zhu J, Liu F, Gong Y, Li Z. Preoperative vitamin D deficiency and postoperative hypocalcemia in thyroid cancer patients undergoing total thyroidectomy plus central compartment neck dissection. Oncotarget 2017; 8: 78113-9.
33. Yamashita H, Noguchi S, Murakami T, Uchino S, Watanabe S, Ohshima A, et al. Calcium and its regulating hormones in patients with graves disease: sex differences and relation to postoperative tetany. Eur J Surg 2000; 166: 924-8.
34. Zhang Y, Zheng W, Huang Y, Chen C. Vitamin D insufficiency predicts susceptibility of parathyroid hormone reduction after total thyroidectomy in thyroid cancer patients. Int J Endocrinol 2021; 2021: 8657918.
35. Amrein K, Scherkl M, Hoffmann M, Neuwersch-Sommeregger S, Köstenberger M, Tmava Berisha A, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr 2020; 74: 1498-513.
38. Lederer DJ, Bell SC, Branson RD, Chalmers JD, Marshall R, Maslove DM, et al. Control of confounding and reporting of results in causal inference studies: guidance for authors from editors of respiratory, sleep, and critical care journals. Ann Am Thorac Soc 2019; 16: 22-8.
39. Gao Y, Xiang L, Yi H, Song J, Sun D, Xu B, et al. Confounder adjustment in observational studies investigating multiple risk factors: a methodological study. BMC Med 2025; 23: 132.
40. Admon AJ, Bohnert ASB, Cooke CR, Taylor SP. Beyond confounding: identifying selection bias in observational pulmonary and critical care research. Ann Am Thorac Soc 2022; 19: 1084-9.
42. Casey C, Hopkins D. The role of preoperative vitamin D and calcium in preventing post-thyroidectomy hypocalcaemia: a systematic review. Eur Arch Otorhinolaryngol 2022; 280: 1555-63.